I received this from one of my healthcare HF managers, worth a read:
Below are 10 key highlights from our calls and research regarding COVID-19 and its economic implications. We have spoken with our portfolio companies / boards of directors, advisory board, FDA, NHS (UK), US government / military
officials, healthcare industry CEOs across all major sectors, major academic / medical institutions, major financial institutions / wealth management platforms, and many others.... if you would like to discuss in detail.
Key Highlights:
(1) Given no existing immunity and a high rate of contagion, we believe that up to 80% of the global population will eventually contract the virus. This will not all happen at once but over the course of several years.
(2) Of those infected, data to-date indicate 80% will be early-stage, 15% mid-stage and 5% critical-stage. Early-stage patients will be asymptomatic or mild enough to not require hospitalization. Mid-stage symptoms appear similar to severe
flu, where most patients will stay at home for two weeks and rest. 5% will be critical and highly weighted toward the elderly.
(3) It is difficult to know the ultimate mortality rate at this point. Once the disease is fully quantified, we think 0.25-0.50% is
realistic, heavily weighted toward the elderly and immune compromised. Treatments / therapeutics will be needed for the sickest, otherwise this figure could increase. In the US, about 3mm people die each year, primarily from old age and nonvirus disease, those two being highly correlated. There will be significant overlap with COVID-19, so this does not mean 600k - 1.3mm new deaths from this virus. Rather, many elderly people will die sooner due to the associated respiratory distress. COVID-19 may, however, put immense pressure on the US healthcare system.
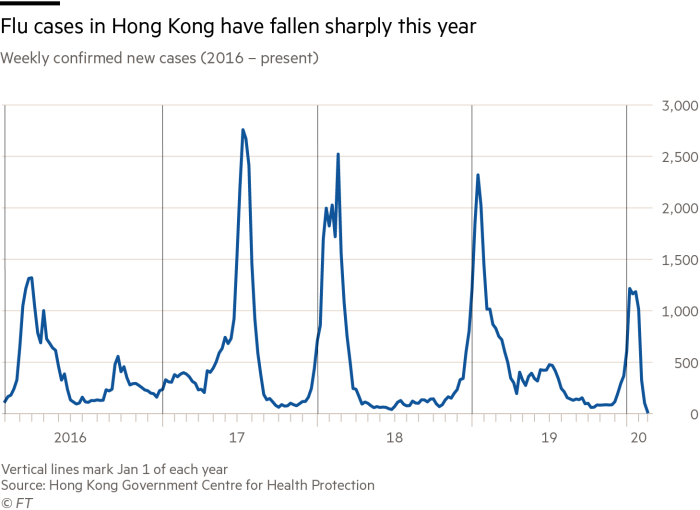
(4) Peak virus is expected in the next 8 weeks (mid-May), and new cases may continue to run through the middle of the summer (mid-July). Like the EU, US peak levels will be determined by geographic containment strategies. The virus is likely seasonal and could reemerge in populations without immunity in the Fall. Reinfection rates are expected to be low, given the lack of virus mutation seen to date. The upside case is that the virus runs its course by early summer. The downside case is that containment is pushed into the Fall or longer.
(5) Most countries now agree that social distancing and quarantine are the best approaches to mitigating transmission. Quarantine may 'flatten the curve' though will result in significant economic damage. It will also slow the rate of transmission allowing the healthcare system time to respond. Herd immunity will be the ultimate solution. In the interim, the medical community must mitigate the damage, there is only so much monetary and fiscal stimulus can do.
(6) Treatment options will come in three waves: (i) currently approved, repurposed therapeutics to minimize near-term mortality (e.g. sarilumab / hydroxychloroquine); (ii) therapeutics in development that will not be available until Fall via
emergency use authorization (e.g. anti-virals like remdesivir / favipravir; antibodies; maybe RNA vaccines); and (iii) standard vaccines that will take 12-18 months.
...Our relationships that provide unique insight into the virus dynamics, e.g.
Dr Schinazi (Emory virologist who invented HCV cure, HIV treatments, and COVID-19 treatments), Sir Bruce Keogh (former head of NHS (UK) who led response to the UK’s 2009 swine flu outbreak, Don Berwick (former head of Center for Medicaid & Medicare Services (US)), The Gates Foundation, and many others.'